

The S c i e n c e of :
O p i o i d A d d i c t i o n
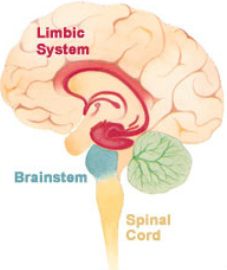
Opioid dependency is classified as a true medical condition and is the direct result of dramatic brain structure changes. Once these brain structure changes take hold, an individual is no longer left with an easy choice to"simply not use", but is faced with an overpowering & persistent desire to feed an opioid drug hunger. No one wants to become addicted. Remember, the person did not want this to happen.
This overpowering urge is a phenomenon that most non-addicted people have difficulty understanding. People often naively ask "Why can't they just stop?" If it were that easy, they would! For an opioid dependent individual, the overpowering urge to use is very similar to a typical person experiencing extreme hunger after not eating for a prolonged period of time. The longer one goes without food, more intense becomes their physical discomfort, and the hungry person becomes sharply focused on finding something to eat. This is a powerful physiological drive that blocks out other goals & considerations .....until the need is met.
Another illustration is a person severely dehydrated and overcome with the desire to take in fluids. When they get to water, they rapidly gulp it down trying to satisfy their extreme thirst. Yet another example is the powerful sleep mechanism which kicks in after many hours wide awake. If you have ever watched someone fight sleep, you will inevitably see them give in to sleep as the body's physiological need overcomes the individual's intention to remain awake.
And such is the case with a physiological dependency on opioids. The drive to use becomes increasingly powerful and eventually overwhelms the addicted individual. Due to structural changes within the brain, the brain begins to crave opiates like people crave food, water, and sleep. And just as someone becomes intensely symptomatic when deprived of food, water, or sleep, the opioid dependent person becomes increasingly sick from opioid withdrawal, and desperate to end their physical discomfort.
---> H O W A D D I C T I O N D E V E L O P S <---

<1> Introduction.
Addiction often begins with a legitimate opioid prescription for temporary pain relief,
or brief experimental use for recreational purposes (such as taking a friend's pain pill).
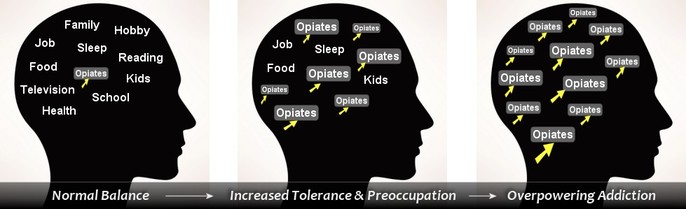
<2> Rewards.
The individual discovers that the opiate/opioid successfully controls pain or provides a
sense of euphoria or pleasure. As use of the opioid continues, cell adaptation occurs and
tolerance to the opioid begins to grow. This requires larger amounts of the opioid in order to achieve the same effect.
<3>Nightmare Begins...
For some people, a physical dependency can come about quickly. For others, it may take longer. Once physically "hooked", the person then
goes thru severe,uncomfortable withdrawal symptoms as the effect of the
opioid wears off. what occurs next??
An intense drug craving develops.
<4> Your 'New' Reality.
The person's discomfort is immediately relieved by taking more &
more of the drug. They do this, and the addictive cycle worsens
grows, and eventually takes over and becomes long-term and in most cases becomes their LIFE, and will BE a LIFE -LONG PROBLEM.
Addiction often begins with a legitimate opioid prescription for temporary pain relief,
or brief experimental use for recreational purposes (such as taking a friend's pain pill).
<2> Rewards.
The individual discovers that the opiate/opioid successfully controls pain or provides a
sense of euphoria or pleasure. As use of the opioid continues, cell adaptation occurs and
tolerance to the opioid begins to grow. This requires larger amounts of the opioid in order to achieve the same effect.
<3>Nightmare Begins...
For some people, a physical dependency can come about quickly. For others, it may take longer. Once physically "hooked", the person then
goes thru severe,uncomfortable withdrawal symptoms as the effect of the
opioid wears off. what occurs next??
An intense drug craving develops.
<4> Your 'New' Reality.
The person's discomfort is immediately relieved by taking more &
more of the drug. They do this, and the addictive cycle worsens
grows, and eventually takes over and becomes long-term and in most cases becomes their LIFE, and will BE a LIFE -LONG PROBLEM.
|


 
VICODIN (hydrocodone/apap)
|
|

The C h a n g i n g F a c e of
O p i o i d A d d i c t i o n
Addiction to opiates as far as we know began to change in the early 20th century with the arrival of waves of European immigrants.
Most users of opioids were young men in their 20s: down-and-outs of recent-immigrant European stock who were crowded into tenements and ghettos and became addicted during adolescence or early adulthood.
They often resorted to illegal means to obtain their opioids.
*The initial treatment response in the early 20th century involved prescribing short-acting opioids.
By the 1920s, morphine was prescribed or dispensed in treatment programs.
*Addictive use of opium, cocaine, and heroin, along with drug-related crime, especially in urban communities, increasingly concerned social, religious, and political leaders.
Negative attitudes toward, and discrimination against, new immigrants probably influenced views of addiction.
Society‘s response was to turn from rudimentary forms of treatment to law enforcement.
*Another major change in the U.S. opioid-addicted population occurred after World War II.
As many European immigrants moved from crowded cities, Hispanics and African Americans moved into areas with opioid use problems, and the more susceptible people in these groups acquired the disorder.
*The post-World War II shift in the composition of opioid-addicted groups
coincided with hardening attitudes toward these groups.
*By the 1980s, an estimated 500,000 Americans used illicit opioids (mainly heroin).
Although this number represented a 66-percent increase over the estimated number of late 19th-century
Americans with opioid addiction, the per capita rate was much less than in the
late 19th century because the population had more than doubled.
Nevertheless, addiction became not only a major medical problem but also an explosive social issue.
*By the late 1990s, 898,000 people in the United States used heroin,
and the number seeking treatment was approximately 200,000
(almost double the number during the 1980s).
*Year 2000, The abuse of prescription opioids was a growing concern.
Treatment admission rates for addiction to opioid analgesics more than doubled between 1992 and 2001,
and emergency room visits related to opioid analgesic abuse increased 117 percent between 1994 and 2001.
* Year 2011, Opioid-dependence has grown to epidemic proportions.
This disease has affected every race, socio-economic class, every gender, every profession.
This drug knows NO boundaries.
New treatments including Suboxone are now offered and new laws are in the
process of being made to help end this nightmare of an issue.
7 out of Ten families are effected Directly.
Opioids are today's what marijuana was to the 60's.
*Between 500,000 and One Million People in America are Believed to be
Opioid dependent at any given time.
. . . To Be Continued. . .

|
|
OxyContin: Recognize The Demon
|
THE DRUG ADDICTION TREATMENT ACT OF 2000
(DATA 2000)
The Drug Addiction Treatment Act of 2000 (DATA 2000)The Drug Addiction Treatment Act of 2000 (DATA 2000) expands the clinical context of medication-assisted opioid addiction treatment by allowing qualified physicians to dispense or prescribe specifically approved Schedule III, IV, and V narcotic medications for the treatment of opioid addiction in treatment settings other than the traditional Opioid Treatment Program (i.e., methadone clinic). In addition, DATA 2000 reduces the regulatory burden on physicians who choose to practice opioid addiction therapy by permitting qualified physicians to apply for and receive waivers of the special registration requirements defined in the Controlled Substances Act.
To Learn More About This Law Click on Picture :
(Link will take you to different site in new window)
www.buprenorphine.samhsa.gov/data.html
To Learn More About This Law Click on Picture :
(Link will take you to different site in new window)
www.buprenorphine.samhsa.gov/data.html
 <><><><><><><><><><><><><><><>
F A C T S O N O P I O I D U S E
A N D I T S E F F E C T S Opiate Overdose The main cause of death resulting from overdoses of opiate type drugs such as heroin, morphine or codeine is ‘depressed’ breathing ( slow, shallow breathing which can potentially lead to unconsciousness and then death ) which is caused by a lack of oxygen reaching the body. Opioids suppress activity in the brain causing the body to lose its ability to react to the chemical changes ( such as the harmful levels of carbon dioxide ) which would usually trigger the mechanisms responsible for breathing. Depressed breathing can also cause excess fluid in the lungs which is called pulmonary edema. This can happen either gradually or else so quickly that this in itself can be a direct cause of death. If someone has taken an overdose of an opiate drug, it is most probable that the pupils of their eyes will contract and become like pinpoints and that they will be displaying extreme lethargy if not already in a coma. Prolonged depressed breathing may result in extremely low blood pressure and dilated (enlarged) pupils. Quickly restoring their ability to breathe properly is the key to their resuscitation and ultimately their survival. It is for this reason that it is particularly dangerous when a person is alone as there is no-one there to summon help on their behalf when they fall into a state of unconsciousness. Whilst it is true that drug users can develop a ‘tolerance’ to many effects of the opioid drugs they are regularly taking, developing a tolerance to respiratory depression is a much slower process and even heavy or prolonged use does not mean that the drug taker is any less susceptible to falling victim to a death caused by depressed breathing. In a clinical environment, medical staff can administer an antidote to heroin overdose. This drug is called naloxone and is an opiate antagonist. This means that the drug replaces the opiates which are bound to receptors in the person's brain. This causes instant withdrawal, but prevents the respiratory suppression caused by the opiate overdose. CONTINUED TOP RIGHT COLUMN --> D O C U M E N T A R Y:
* H e r o i n : The Next Generation *
|
O P I O I D A D D I C T I O N &
O P I O I D W I T H D R A W A L S Y M P T O M S : When addicted to opiates, such as heroin, the drug must be taken regularly or else withdrawal symptoms will begin - hence the addiction. Such symptoms of withdrawal can include mood swings, irritability, head aches, nausea, cramps, sweating, trembling and more. Whilst extremely unpleasant, opiate withdrawal is not fatal. It is opiate drug overdose which is responsible for the most drug related deaths. "Cold Turkey" is a term used when an opiate addict attempts to discontinue their useof opiates, ultimately resulting in withdrawal. In comparison to 'weaning' off of the opiates, they just 'stop'. Unfortunately, statistics show that only 5% of those who choose this method of treatment- are successful. Types of Opiates There are a number of different types of opiate based drugs. These include both illegal drugs such as heroin and opium, along with prescription opiates such as morphine and dihydrocodeine, and over-the-counter opiates such as codeine. How long do opiates stay in your system? Opiates are typically detectable in a person's urine for 2 - 4 days, perhaps as long as 5 days at the outside. This is based upon the standard cut-off level of 300ng/ml used in Europe. In the USA, where a 2000ng/ml level is commonly used, this retention time is slightly less. Opiates in urine are detectable for a much shorter time than in hair. Hair testing can detect opiate abuse for months after use - dependent on the length of the person's hair source: drug-aware.com 
|
Medication Assisted Treatment for Opioid Addiction :
June 'Challenges and Solutions' 2011

*FACT:
*Between 1990 and 2001, the number of people who used prescription painkillers recreationally for the first time grew by 335% to include almost 2.5 million people*
and...DiD yOu kNoW?
*Afghanistan produces 90 percent of the world’s supply of opium, the raw ingredient used to make heroin.
Pasted from <http://blog.opiates.com/>
and...DiD yOu kNoW?
*Afghanistan produces 90 percent of the world’s supply of opium, the raw ingredient used to make heroin.
Pasted from <http://blog.opiates.com/>
Statistics from:
U.S. Department of Health and Family Services
* Prescription * Medication *
a b u s e & a d d i c t i o n
[-] In 2006, an estimated 20.4 million Americans
aged 12 or older were current (past month) illicit Prescription users, meaning they had used
illicit Prescription during the month prior to the survey interview.
This estimate represents 8.3 percent of the population aged 12 years old or older.
Illicit drugs include Prescription/hashish, Prescription (including Prescription), heroin, hallucinogens, Prescription, or prescription-type psychotherapeutics used non-medically.
[-]In 2006, there were 2.4 million current Prescription users aged 12 or older,
which was the same as in 2005 but greater than in 2002 when the number was 2.0 million.
However, the rate of current Prescription use remained stable between 2002 and 2006.
[-] Hallucinogens were used in the past month by 1.0 million
persons aged 12 or older in 2006,
including 528,000 who had used Prescription.
These estimates are similar to the corresponding estimates for 2005.
[-] There were 7.0 million persons aged 12 or older who used
prescription-type psychotherapeutic drugs non-medically in the past month.
Of these, 5.2 million used pain relievers, an increase from 4.7 million in 2005.
[-] In 2006, there were an estimated 731,000 current users of Prescription aged 12 or older.
[-] Among youths aged 12 to 17,
current illicit Prescription use rates remained stable from 2005 to 2006.
However, youth rates declined significantly between 2002 and 2006
for illicit drugs in general and for several specific drugs,
including Prescription, hallucinogens, prescription-type drugs used non-medically,
pain relievers, tranquilizers, and the use of illicit drugs other than Prescription.
[-] The rate of current Prescription use among youths aged 12 to 17
declined from 8.2 percent in 2002 to 6.7 percent in 2006.
[-] Among persons aged 12 or older who used pain relievers non-medically in the past 12 months,
55.7 percent reported that the source of the Prescription the most recent time they
used was from a friend or relative for free.
SOURCE: http://www.drug-addiction-support.org/Opioid-Abuse-Facts.html
aged 12 or older were current (past month) illicit Prescription users, meaning they had used
illicit Prescription during the month prior to the survey interview.
This estimate represents 8.3 percent of the population aged 12 years old or older.
Illicit drugs include Prescription/hashish, Prescription (including Prescription), heroin, hallucinogens, Prescription, or prescription-type psychotherapeutics used non-medically.
[-]In 2006, there were 2.4 million current Prescription users aged 12 or older,
which was the same as in 2005 but greater than in 2002 when the number was 2.0 million.
However, the rate of current Prescription use remained stable between 2002 and 2006.
[-] Hallucinogens were used in the past month by 1.0 million
persons aged 12 or older in 2006,
including 528,000 who had used Prescription.
These estimates are similar to the corresponding estimates for 2005.
[-] There were 7.0 million persons aged 12 or older who used
prescription-type psychotherapeutic drugs non-medically in the past month.
Of these, 5.2 million used pain relievers, an increase from 4.7 million in 2005.
[-] In 2006, there were an estimated 731,000 current users of Prescription aged 12 or older.
[-] Among youths aged 12 to 17,
current illicit Prescription use rates remained stable from 2005 to 2006.
However, youth rates declined significantly between 2002 and 2006
for illicit drugs in general and for several specific drugs,
including Prescription, hallucinogens, prescription-type drugs used non-medically,
pain relievers, tranquilizers, and the use of illicit drugs other than Prescription.
[-] The rate of current Prescription use among youths aged 12 to 17
declined from 8.2 percent in 2002 to 6.7 percent in 2006.
[-] Among persons aged 12 or older who used pain relievers non-medically in the past 12 months,
55.7 percent reported that the source of the Prescription the most recent time they
used was from a friend or relative for free.
SOURCE: http://www.drug-addiction-support.org/Opioid-Abuse-Facts.html


The following Opiate-based drugs will produce a positive result on an Opiate drug test:
|
OTC List of the more common medications available
|
|
Aspirin and Codeine Tablets BP
MXL Capsules Benylin with Codeine Nurofen Plus Oramorph Boots Tension Headache Relief Panadol Ultra Co-codamol Paracodol Codafen Continus Paramol Tablets Codeine Sulphate Propain Tablets Codis 500 Pulmo Bailly Cyclimorph Injection Remedeine Dimotane Co DHC Continus MSA Continus Suspension / Tablets ___________________________________ F A C T : *DiD You Know? --> Oxycodone, Methadone, & Fentanyl WILL NOT Show Up On Standard Drug Tests . |
Remedeine Forte Tablets
Robitussin Night-Time Dihydrocodeine Sevredol Oral Solution Diocalm Solpadeine DF118 Solpadeine MAX Famel Original Cough Syrup Solpadeine Solpadeine Oral Solution Feminax Solpadol Capsules / Effervescent / Caplets J Collis Browne’s Mixture / Tablets Solpaflex tablets Kapake Syndol Tylex Capsules / Effervescent Migraleve Pink/ Migraleve Yellow Veganin Tablets Zomorph _____________________________________________________ AnD... Standard Tests Are What The MAJORITY of Employers, etc. Use. EACH of those 3 Opioids have individual tests that are needed to detect their presence & are Quite Expensive. |
*F A C T :
*According to Time Magazine, Vicoden was prescribed
131.2 million times in 2010,
an increase of exactly 3 million from the year before (2009).
131.2 million times in 2010,
an increase of exactly 3 million from the year before (2009).
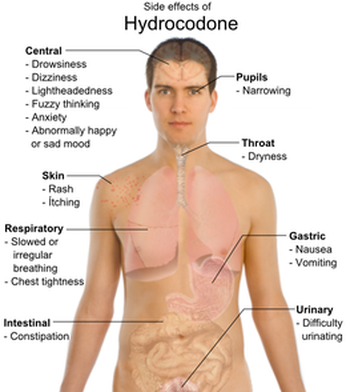
What Is Hydrocodone ?
a.k.a
(Vicoden, Lortab/Lorcet, Norco, Hydros, dros, tabs)
(hi.dro.co.doe'n)

Hydrocodone or dihydrocodeinone is a semi-synthetic opioid derived from two of the naturally occurring opiates, codeine and thebaine. Hydrocodone is an orally active narcotic analgesic (pain reliever) and antitussive (cough suppressant). It is commonly available in tablet, capsule, and syrup form, and is often compounded with other analgesics like paracetamol or ibuprofen.
Hydrocodone is marketed, in its varying forms, under a number of trademarks, including Vicodin, Symtan, Anexsia, Dicodid, Hycodan (or generically Hydromet), Hycomine, Hycet, Lorcet, Lortab, Norco, Novahistex, Hydrovo, Duodin, Kolikodol, Orthoxycol, Mercodinone, Synkonin, Norgan, and Hydrokon. Hydrocodone was first synthesized in Germany in 1920[1] and was approved by the Food and Drug Administration on 23 March 1943 for sale in the United States and Canada under the brand name Hycodan.[2][3]
The particular niche in which hydrocodone is most commonly used is as an intermediate strength centrally acting analgesic and strong cough suppressant, especially in those for whom histamine release and attendant itching from codeine is a problem. For the latter indication, at the 5 to 10 mg dose range hydrocodone is more powerful than most cough suppressants, being roughly equal to its derivative dihydrocodeinone enol acetate, with the top of the list being morphine and hydromorphone (Dilaudid cough syrup) and methadone (methadone linctus, about 33 percent the concentration of the liquid used for opioid physical dependence maintenance or detoxification) and dihydrocodeine being right below. The experiments in dogs conducted by Winder and Rosière in the mid-1950s reported in the Journal of Pharmacology in 1955 indicate that hydrocodone is 12 times stronger than codeine as an antitussive (morphine 14x, methadone 9x), and other tests from 1920 forward showed it was about six times stronger as an analgesic.
Hydrocodone is marketed, in its varying forms, under a number of trademarks, including Vicodin, Symtan, Anexsia, Dicodid, Hycodan (or generically Hydromet), Hycomine, Hycet, Lorcet, Lortab, Norco, Novahistex, Hydrovo, Duodin, Kolikodol, Orthoxycol, Mercodinone, Synkonin, Norgan, and Hydrokon. Hydrocodone was first synthesized in Germany in 1920[1] and was approved by the Food and Drug Administration on 23 March 1943 for sale in the United States and Canada under the brand name Hycodan.[2][3]
The particular niche in which hydrocodone is most commonly used is as an intermediate strength centrally acting analgesic and strong cough suppressant, especially in those for whom histamine release and attendant itching from codeine is a problem. For the latter indication, at the 5 to 10 mg dose range hydrocodone is more powerful than most cough suppressants, being roughly equal to its derivative dihydrocodeinone enol acetate, with the top of the list being morphine and hydromorphone (Dilaudid cough syrup) and methadone (methadone linctus, about 33 percent the concentration of the liquid used for opioid physical dependence maintenance or detoxification) and dihydrocodeine being right below. The experiments in dogs conducted by Winder and Rosière in the mid-1950s reported in the Journal of Pharmacology in 1955 indicate that hydrocodone is 12 times stronger than codeine as an antitussive (morphine 14x, methadone 9x), and other tests from 1920 forward showed it was about six times stronger as an analgesic.
 |
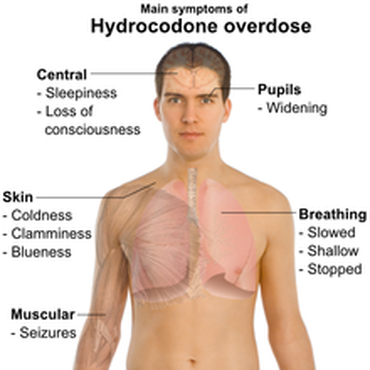 Symptoms Of Hydrocodone Overdose |
*F A C T:
---> In The Year 2000 , There Were Over 89 MILLION Prescriptions for
Hydrocodones written in the United States.*


Pharmacology Of Hydrocodones:

~Hydrocodone Bitartrate~
As a narcotic, hydrocodone relieves pain by binding to opioid receptors in the brain and spinal cord. It can be taken with or without food as desired. When taken with alcohol, it can intensify drowsiness. It may interact with monoamine oxidase inhibitors, as well as other drugs that cause drowsiness. It is in FDA pregnancy category C: Animal reproduction studies have shown an adverse effect on the fetus, and there are no adequate and well-controlled studies in humans, but potential benefits may warrant use of the drug in pregnant women despite potential risks. In addition, a newborn of a mother taking the medication may exhibit breathing problems or withdrawal symptoms.
Studies have shown hydrocodone as stronger than codeine but only one-tenth as potent as morphine at binding to receptors, whereas roughly half as potent as morphine in analgesic properties. However other studies have shown hydrocodone to be anywhere from half as potent to oxycodone (1.5× the potency of morphine) to only 66.6~% the potency of oxycodone (equipotent to morphine). Hydrocodone can be habit-forming, which leads to physical and psychological dependence, but the potential for addiction varies from individual to individual depending on unique biological differences. Sales and production of this drug have increased significantly in recent years, as have diversion and illicit use. In the U.S., formulations containing more than 15 mg per dosage unit are considered Schedule II drugs, as would any formulation consisting of just hydrocodone alone (however the latter do not exist in the U.S.). Those containing less than or equal to 15 mg per dosage unit in combination with acetaminophen or another non-controlled drug are called hydrocodone compounds and are considered Schedule III drugs. Hydrocodone is typically found in combination with other drugs such as paracetamol, aspirin, ibuprofen and homatropine methylbromide.
The purpose of the non-controlled drugs in combination is often twofold:
1.) To provide increased analgesia via drug synergy.
2.) To limit the intake of hydrocodone by causing unpleasant and often unsafe side effects at higher-than-prescribed doses.
In the UK, it is listed as a Class A drug under the Misuse of Drugs Act 1971. Hydrocodone is not available in pure form in the United States due to a separate regulation, and is always sold with an NSAID, acetaminophen, antihistamine, expectorant, or homatropine. The cough preparation Codiclear DH is the purest US hydrocodone item, containing guaifenesin and small amounts of ethanol as active ingredients. In Germany and elsewhere, hydrocodone is available as single-active-ingredient tablets as Dicodid (by analogy to the original manufacturer's other products Dilaudid and Dinarkon and others) available in 5- and 10-mg strengths.
As with many other opioids, it is quite possible to reduce the amount of hydrocodone needed to stop a certain level of pain by having the patient take the hydrocodone along with one of the medications with analgesic-sparing properties, also known as potentiators. The most common, one of the most effective with hydrocodone, and safest is hydroxyzine. Orphenadrine, nefopam, carisoprodol, and antihistamines also potentiate most opioids. Especially in the case of carisoprodol, it is imperative that the titration and addition of the potentiator be done under strict supervision of a physician.
Hydrocodone also interacts relatively well with most adjuvant and atypical analgesics used for severe and neuropathic pain such as first-generation anti-depressants, anticholinergics, anticonvulsants, centrally acting stimulants, NMDA antagonists, etc. Hydrocodone can usually be successfully used with duloxetine (Cymbalta) for neuropathic pain, especially that from diabetic neuropathy, provided that the patient has normal relative and absolute levels of Cytochrome P450-related liver enzymes.
Studies have shown hydrocodone as stronger than codeine but only one-tenth as potent as morphine at binding to receptors, whereas roughly half as potent as morphine in analgesic properties. However other studies have shown hydrocodone to be anywhere from half as potent to oxycodone (1.5× the potency of morphine) to only 66.6~% the potency of oxycodone (equipotent to morphine). Hydrocodone can be habit-forming, which leads to physical and psychological dependence, but the potential for addiction varies from individual to individual depending on unique biological differences. Sales and production of this drug have increased significantly in recent years, as have diversion and illicit use. In the U.S., formulations containing more than 15 mg per dosage unit are considered Schedule II drugs, as would any formulation consisting of just hydrocodone alone (however the latter do not exist in the U.S.). Those containing less than or equal to 15 mg per dosage unit in combination with acetaminophen or another non-controlled drug are called hydrocodone compounds and are considered Schedule III drugs. Hydrocodone is typically found in combination with other drugs such as paracetamol, aspirin, ibuprofen and homatropine methylbromide.
The purpose of the non-controlled drugs in combination is often twofold:
1.) To provide increased analgesia via drug synergy.
2.) To limit the intake of hydrocodone by causing unpleasant and often unsafe side effects at higher-than-prescribed doses.
In the UK, it is listed as a Class A drug under the Misuse of Drugs Act 1971. Hydrocodone is not available in pure form in the United States due to a separate regulation, and is always sold with an NSAID, acetaminophen, antihistamine, expectorant, or homatropine. The cough preparation Codiclear DH is the purest US hydrocodone item, containing guaifenesin and small amounts of ethanol as active ingredients. In Germany and elsewhere, hydrocodone is available as single-active-ingredient tablets as Dicodid (by analogy to the original manufacturer's other products Dilaudid and Dinarkon and others) available in 5- and 10-mg strengths.
As with many other opioids, it is quite possible to reduce the amount of hydrocodone needed to stop a certain level of pain by having the patient take the hydrocodone along with one of the medications with analgesic-sparing properties, also known as potentiators. The most common, one of the most effective with hydrocodone, and safest is hydroxyzine. Orphenadrine, nefopam, carisoprodol, and antihistamines also potentiate most opioids. Especially in the case of carisoprodol, it is imperative that the titration and addition of the potentiator be done under strict supervision of a physician.
Hydrocodone also interacts relatively well with most adjuvant and atypical analgesics used for severe and neuropathic pain such as first-generation anti-depressants, anticholinergics, anticonvulsants, centrally acting stimulants, NMDA antagonists, etc. Hydrocodone can usually be successfully used with duloxetine (Cymbalta) for neuropathic pain, especially that from diabetic neuropathy, provided that the patient has normal relative and absolute levels of Cytochrome P450-related liver enzymes.
* MORE THEN ADDICTION:
| |||










| recoveryrights.pdf |
Opiate Addiction:
Fear Of ‘Drug Sickness’ Keeps
Addicts Using
Opiate addiction and the need for opiate treatment is definitely on the rise. But these days it is not in the traditional form of heroin, but rather in the form of prescription pill medication. Prescription pain killers are a segment of drug use that is rising astronomically.
It is now not uncommon in alcohol and drug rehab’s to have groups with 50% of the people either abusing or addicted to opiates. And within this group of people one of the most common fears verbalized is fear of drug sickness. This is not the usual unpleasant effects of with drawl that are described by other users.
Withdrawal from opiates while as dangerous in a medical sense, as withdrawal from alcohol or benzodiazepines, can be very unpleasant and prolonged.
So the concept of getting high and stay high becomes cemented in
the mine of an opiate user not from the desired to feel the effects of the high, but to avoid negative effects of the withdrawal. This is an extremely powerful motivator for continued use.
There is a high rate of opiate users needing treatment for the end
of the program because the fear of the withdrawals becomes so great that they feel they must use. Getting through an opiate withdrawal can be described in the sense of getting over the hump. There is great discomfort and then there is a breakthrough moment. Unfortunately, many people eat before they have the breakthrough.
Fortunately, there is some government approved medication that can help with the unpleasant effects of opiate withdrawal; Buprenorphine and Methadone.
That is the good news.
The bad news is that there are so many misconceptions about their use, and effectiveness. People stereotype the use of these medications as trading in one addiction for another. It’s the lack
of knowledge and education about these treatments that is the #1
problem.
With the rates of pain pill addiction skyrocketing it is essential that we get the correct information out to people in every community, both large cities and the small rural areas as well..
The rich, the poor, the college graduates, the dropouts, the fast
food worker, even your mayor can fall victim to the devastating effects of opiate addiction.
NOBODY is immune.
It is now not uncommon in alcohol and drug rehab’s to have groups with 50% of the people either abusing or addicted to opiates. And within this group of people one of the most common fears verbalized is fear of drug sickness. This is not the usual unpleasant effects of with drawl that are described by other users.
Withdrawal from opiates while as dangerous in a medical sense, as withdrawal from alcohol or benzodiazepines, can be very unpleasant and prolonged.
So the concept of getting high and stay high becomes cemented in
the mine of an opiate user not from the desired to feel the effects of the high, but to avoid negative effects of the withdrawal. This is an extremely powerful motivator for continued use.
There is a high rate of opiate users needing treatment for the end
of the program because the fear of the withdrawals becomes so great that they feel they must use. Getting through an opiate withdrawal can be described in the sense of getting over the hump. There is great discomfort and then there is a breakthrough moment. Unfortunately, many people eat before they have the breakthrough.
Fortunately, there is some government approved medication that can help with the unpleasant effects of opiate withdrawal; Buprenorphine and Methadone.
That is the good news.
The bad news is that there are so many misconceptions about their use, and effectiveness. People stereotype the use of these medications as trading in one addiction for another. It’s the lack
of knowledge and education about these treatments that is the #1
problem.
With the rates of pain pill addiction skyrocketing it is essential that we get the correct information out to people in every community, both large cities and the small rural areas as well..
The rich, the poor, the college graduates, the dropouts, the fast
food worker, even your mayor can fall victim to the devastating effects of opiate addiction.
NOBODY is immune.
___________________________________
---> STAGES
o f
SUBSTANCE ABUSE <---
___________________________________

Experimentation, regular use, risky use, dependence, and addiction are the stages of substance use.
Related behaviors can be addressed and treated, if necessary, at any stage – despite popular myths, people do not need to “hit bottom” or become addicted before they can benefit from help.
1. EXPERIMENTATION
Substance use starts with experimentation -- or the voluntary use of alcohol or other drugs. Frequently, the person experimenting is trying to erase another problem. An older person may self-medicate by drinking to cope with depression after losing a spouse. A teenager, angry about his parents’ divorce, could start smoking marijuana or huffing inhalants. Experimentation may even include a husband taking his wife’s prescription painkillers to cope with a back problem.
In all of these cases, the substance seems to solve the problem. So the person takes more, and moves from experimentation to regular use, the next stage. Some people will stay in this stage indefinitely, will not develop a problem, and will probably stop by themselves. But others will start using substances in a manner that is risky or hazardous to themselves or to others. Smoking marijuana and driving is an example of a risky behavior. Or having unprotected sex. So is binge drinking (having more than the recommended amount of alcohol at one occasion).
3. REGULAR USE
&
4. RISKY USE
If, when, and how the transition from regular to risky use happens differs for every individual. And while it doesn’t happen to everyone, the National Institute on Alcohol Abuse and Alcoholism (NIAAA) estimates that nearly one-third of Americans engage in risky drinking patterns
As a result, what constitutes “risky behavior” by another person can be difficult to gauge — unless it’s obvious, of course. If someone’s behavior worries you, you owe it to yourself and them to say something. The slope from risky behavior to dependence is slippery, and there are interventions for risky users that can reduce harm.
4. DEPENDENCE
Alcohol or drug dependence follows risky behavior. According to Maryann Amodeo, Director of the Alcohol and Drug Institute for Policy, Training and Research at Boston University, the characteristics of dependence include:
1.) Repeated use of alcohol or other drugs leading to failure to fulfill major responsibilities related to work, family, school or other roles
2.) Repeatedly drinking or using drugs in situations that are physically hazardous, such as driving while intoxicated or using heavy machinery when intoxicated
3.) Repeated legal problems
At this stage, alcohol or other drug use may not yet be compulsive and out of control. Many dependent people are able to work, maintain family relationships and friendships, and limit their use of alcohol or other drugs to certain time periods, such as evenings or weekends. But it’s also difficult for them and for others to see the effect their substance use may be having on themselves, friends, and family members. And again, there are appropriate interventions for substance users in this stage, and those around them.
5. ADDICTION
The last phase of the spectrum of substance use problems is addiction. Addiction is a medical condition involving serious psychological and physical changes from repeated heavy use of alcohol, other drugs, or both. The symptoms of addiction are: uncontrollable alcohol or other drug craving, seeking, and use that persists even in the face of negative consequences. It is a progressive illness, meaning it gets worse over time if left untreated. It is also chronic, or long-standing (versus acute, or short-term).
Addiction is also a treatable illness. Recovery rates for people who go through treatment are very similar to those who get treatment for other chronic diseases such as diabetes and asthma. There are a number of treatment methods and community resources, including outpatient or residential treatment programs and twelve-step groups. These approaches can be customized to fit the needs of the individual and family. Learn more about understanding addiction.
And remember: substance use can be addressed before it becomes an addiction or a dependence.
[Source: Mary Ann Amodeo/Join Together]
Related behaviors can be addressed and treated, if necessary, at any stage – despite popular myths, people do not need to “hit bottom” or become addicted before they can benefit from help.
1. EXPERIMENTATION
Substance use starts with experimentation -- or the voluntary use of alcohol or other drugs. Frequently, the person experimenting is trying to erase another problem. An older person may self-medicate by drinking to cope with depression after losing a spouse. A teenager, angry about his parents’ divorce, could start smoking marijuana or huffing inhalants. Experimentation may even include a husband taking his wife’s prescription painkillers to cope with a back problem.
In all of these cases, the substance seems to solve the problem. So the person takes more, and moves from experimentation to regular use, the next stage. Some people will stay in this stage indefinitely, will not develop a problem, and will probably stop by themselves. But others will start using substances in a manner that is risky or hazardous to themselves or to others. Smoking marijuana and driving is an example of a risky behavior. Or having unprotected sex. So is binge drinking (having more than the recommended amount of alcohol at one occasion).
3. REGULAR USE
&
4. RISKY USE
If, when, and how the transition from regular to risky use happens differs for every individual. And while it doesn’t happen to everyone, the National Institute on Alcohol Abuse and Alcoholism (NIAAA) estimates that nearly one-third of Americans engage in risky drinking patterns
As a result, what constitutes “risky behavior” by another person can be difficult to gauge — unless it’s obvious, of course. If someone’s behavior worries you, you owe it to yourself and them to say something. The slope from risky behavior to dependence is slippery, and there are interventions for risky users that can reduce harm.
4. DEPENDENCE
Alcohol or drug dependence follows risky behavior. According to Maryann Amodeo, Director of the Alcohol and Drug Institute for Policy, Training and Research at Boston University, the characteristics of dependence include:
1.) Repeated use of alcohol or other drugs leading to failure to fulfill major responsibilities related to work, family, school or other roles
2.) Repeatedly drinking or using drugs in situations that are physically hazardous, such as driving while intoxicated or using heavy machinery when intoxicated
3.) Repeated legal problems
At this stage, alcohol or other drug use may not yet be compulsive and out of control. Many dependent people are able to work, maintain family relationships and friendships, and limit their use of alcohol or other drugs to certain time periods, such as evenings or weekends. But it’s also difficult for them and for others to see the effect their substance use may be having on themselves, friends, and family members. And again, there are appropriate interventions for substance users in this stage, and those around them.
5. ADDICTION
The last phase of the spectrum of substance use problems is addiction. Addiction is a medical condition involving serious psychological and physical changes from repeated heavy use of alcohol, other drugs, or both. The symptoms of addiction are: uncontrollable alcohol or other drug craving, seeking, and use that persists even in the face of negative consequences. It is a progressive illness, meaning it gets worse over time if left untreated. It is also chronic, or long-standing (versus acute, or short-term).
Addiction is also a treatable illness. Recovery rates for people who go through treatment are very similar to those who get treatment for other chronic diseases such as diabetes and asthma. There are a number of treatment methods and community resources, including outpatient or residential treatment programs and twelve-step groups. These approaches can be customized to fit the needs of the individual and family. Learn more about understanding addiction.
And remember: substance use can be addressed before it becomes an addiction or a dependence.
[Source: Mary Ann Amodeo/Join Together]


|
|
 Video Topic:
|

       |
      FOR ALL THE
|







Disclaimer: The contents of OpioidAddiction.weebly.com/HALO inc. are for general informational purposes only and are not intended to substitute for professional or medical evaluation, diagnosis, treatment, or advice. Users of this site are encouraged to contact your professional healthcare provider for medical assistance regarding addictive disorders, general health problems, mental health problems, and any & all health-related questions.

{kind=link}