
~Oxymorphone - Numorphan - Numorphone - 14-Hydroxydihydromorphinone~
|
|
|
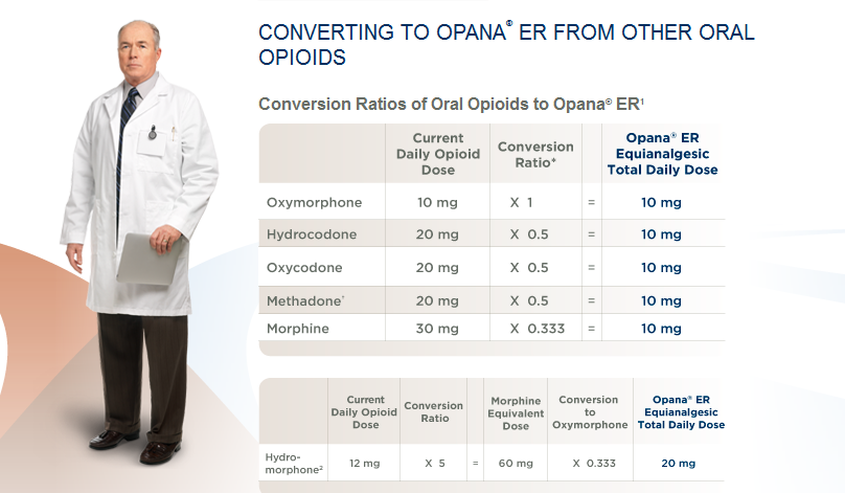
--->What is Opana?
Brand Name: O P A N A Chemical/Generic Name: O X Y M O R P H O N E Oxymorphone is a powerful semi-synthetic opioid analgesic first developed in Germany circa 1914, patented in the USA by Endo Pharmaceuticals in 1955 and introduced to the United States market in January 1959 and other countries around the same time. It (along with hydromorphone) was designed to have less incidence of side effects than morphine and heroin. It was a success as it differs from morphine and heroin in its effects in that it generates less euphoria, sedation, itching and other histamine effects at equianalgesic doses. This also means a lower dependence liability. The brand name Numorphan is derived by analogy to the Nucodan name for an oxycodone product (or vice versa) as well as Paramorphan / Paramorfan for dihydromorphine and Paracodin (dihydrocodeine). The only commercially available salt of oxymorphone in most of the world at this time is the hydrochloride, which has a free base conversion ratio of 0.891. In some countries, hydromorphinol is distributed under the trade names Numorphan and Numorphan Oral. This is a relatively rare exception and the two drugs, whilst both being strong opioid analgesics, are notably different from one another. Oxymorphone is administered as its hydrochloride salt via injection, or suppository; typically in dosages of 1 mg (injected) to 5 mg (suppository). Endo has been the major distributor of oxymorphone throughout the world and currently markets oxymorphone in the United States and elsewhere as Opana and Opana ER. Opana is available as 5 mg and 10 mg tablets; Opana ER, an extended-release form of oxymorphone, is available as tablets in strengths of 5 mg,10 mg, 20 mg, 30 mg, and 40 mg. The 7½ mg and 15 mg strengths of Opana ER have been discontinued as of March 1, 2011. Some resources assert that 2, 12 and/or 15 mg IR tablets and 25, 36 and 50 mg extended release tablets will be introduced although apparently the timeline on that is not known to the public at this time. Opana Extended-Release tablets are based on the TIMERx system developed by a consortium led by Endo and Penwest. Some of these strengths (notably not the 7.5 mg) are available in an Opana IR–immediate release–form for breakthrough pain to be used by patients already on 24/7 opioid care such as fentanyl patches and sustained-relief morphine drugs like Avinza. In addition to the sustained-release version for Opana, other versions of TIMERx are available and being developed for other protocols such as increasing, decreasing, stepwise increasing, and stepwise decreasing dose delivery over time, single and multiple bursts of medication, and combinations of the above. Specifically, the apparent extension of the duration of effect of the IR tablets (all other things being equal, oxymorphone has a duration of action of 5 to 8 hours in most patients) versus similar drugs in commonly used immediate-release forms-for example Dilaudid (hydromorphone),morphine Vilan (nicomorphine), and Paramorfan (dhydromorphne) as well as prodrugs for this group such as hydrocodone, nicocodeine, codeine, dihydrocodeine, and others—is often attributed to marginal extended-release effect from various excipients, particularly those that are hydrophilic and form a gel-like substance at the pH levels in the stomach and duodenum. Both as the result of this and the pharmacokinetics of oxymorphone, the IR tablets have a de facto duration of action of 5 to 13 hours (the mean would seem to be around 7 hours with a moderatly small standard deviation and a left-skewed and leptokurt- ic frequency distribution) in patients with normal kidney and liver function. As a result, patients who go on to extended - release oxymorphone preparations from other opioids may very well need the Opana IR tablets, Numorphan ampoules or phials with hypodermic needles and/or a PCA pump, or immediate-release formulations of hydromorphone, dihydromorphine, high dose oxycodone, nicomorphine hydromorphinol, diamorphine, or morphine for breakthrough pain incidents already in progress. An oxymorphone nasal spray is reportedly in development, along with a possible hydromorphone nasal spray and implantable osmotic pumps for both drugs. The duration of action and metabolic half-life of oxymorphone mean that immediate-release tablets are more similar to analgesic preparations of methadone, levorphenol, piritramide, and existing extended-release forms of morphine, oxycodone, ketobimodone and so on. The extended-release Opana tablets can provide detectable analgesia for anywhere from 6 to 36+ hours (the mean appears to be very close to the lower end of the continuum), largely contingent on things that can alter the drug's liberation, absorption, distribution, metabolism, and elimination profile. One cause is unusual conditions in the upper and middle GI tract, such as created by misoprostol and Arthrotec (misoprostol plus diclofenac). Among other things, misoprostol is a smooth muscle agent with both a contact and systemic mucousagogue that coats the stomach and adjacent areas with increasing amounts of mucus. This can result in everything from even slower onset of action to intact tablets being passed with stool. Oxymorphone is also produced within the human body when the liver metabolises oxycodone by means of O demethylation catalysed by the CYP2D6 enzyme. Approximately 10% of the dose is processed by the endocrine system in this respect; this can vary widely from person to person. The codeine-hydrocodone group and morphinans exhibit the same characteristics. Consuming alcohol with Opana extended-release tablets can be an extremely dangerous situation. The absorption of oxymorphone can vary wildly in the presence of alcohol. Plasma concentrations were found to be as low as 50% of expected to as much as 270% more than expected. Elevated plasma levels could result in overdose. Opana ER does not cause "dose dumping," which creates a blast of drug release that plagues other long acting opioids.- --------------------------------------------------------------------------------------  O p i a t e s
|
|
ARTICLE:
Local P O L I C E Fighting The R I S E in Opana A B U S E |

|
...........................................................
POSTED: 5:05pm EST March 04, 2011
UPDATED: 5:33pm EST March 04, 2011
LOUISVILLE, Ky. -- Local police are fighting a new opponent they said is stronger than oxycontin and oxycodone.Drug task forces on both sides of the river are gearing up to fight the misuse of Opana. Opana, or oxymorphone, is a painkiller like many others, but it's much stronger. However, it's not its strength that's made this drug so popular on the streets; it's actually a recent change in oxycontin that's made Opana an easier drug to misuse -- and a deadlier one."We knew this was going to happen.
Back in November of 2010, oxycontin actually changed its formula because it was being abused so much and tampered with," said Sgt. Jerry Goodin of Indiana State Police."People were crushing it, snorting it, injecting it. Now it's formulated so you cannot do that. So on the street, it doesn't have much value," said Dr. Mark Jorrisch of a Methadone/Opiate Rehabilitation Center. "We knew that our drug abusers would try to find alternatives to that drug."Opana, an extended-release formula of oxymorphone, can be crushed. It's become such a commodity for abusers, many pharmacies in the metro area will not carry it."We've got a river that separates us, but there's a lot of people from Kentucky that go to Indiana, and people from Indiana that go to Kentucky. A lot of our drug dealers cross the river back and forth," said Goodin.
It's also killing people.
Last month, police found pro golfers, Casey Combs and Kenneth Postlewait, dead in an apartment on Taylorsville road. The coroner's report on both men showed substance intoxication, including oxymorphone and alcohol, led to their deaths. But that's just two of several deaths, according to police, in recent months.
WLKY called several local police departments and they were all very aware of Opana.One St. Matthews pharmacy said they had recently been robbed twice by drug abusers looking for opiates like Opana.
Copyright 2011 by WLKY.com. ©2011 Hearst Properties Inc.
Read more: http://www.wlky.com/health/27084156/detail.html#ixzz1WL5nhCij
UPDATED: 5:33pm EST March 04, 2011
LOUISVILLE, Ky. -- Local police are fighting a new opponent they said is stronger than oxycontin and oxycodone.Drug task forces on both sides of the river are gearing up to fight the misuse of Opana. Opana, or oxymorphone, is a painkiller like many others, but it's much stronger. However, it's not its strength that's made this drug so popular on the streets; it's actually a recent change in oxycontin that's made Opana an easier drug to misuse -- and a deadlier one."We knew this was going to happen.
Back in November of 2010, oxycontin actually changed its formula because it was being abused so much and tampered with," said Sgt. Jerry Goodin of Indiana State Police."People were crushing it, snorting it, injecting it. Now it's formulated so you cannot do that. So on the street, it doesn't have much value," said Dr. Mark Jorrisch of a Methadone/Opiate Rehabilitation Center. "We knew that our drug abusers would try to find alternatives to that drug."Opana, an extended-release formula of oxymorphone, can be crushed. It's become such a commodity for abusers, many pharmacies in the metro area will not carry it."We've got a river that separates us, but there's a lot of people from Kentucky that go to Indiana, and people from Indiana that go to Kentucky. A lot of our drug dealers cross the river back and forth," said Goodin.
It's also killing people.
Last month, police found pro golfers, Casey Combs and Kenneth Postlewait, dead in an apartment on Taylorsville road. The coroner's report on both men showed substance intoxication, including oxymorphone and alcohol, led to their deaths. But that's just two of several deaths, according to police, in recent months.
WLKY called several local police departments and they were all very aware of Opana.One St. Matthews pharmacy said they had recently been robbed twice by drug abusers looking for opiates like Opana.
Copyright 2011 by WLKY.com. ©2011 Hearst Properties Inc.
Read more: http://www.wlky.com/health/27084156/detail.html#ixzz1WL5nhCij
New Oxycontin® Formula Prevents Abuse But Lacks Potency
OxyContin®
In 1995, approved by the FDA as a sustained-release preparation of oxycodone hydrochloride and was thought to have much lower abuse potential than immediate-release oxycodone because of its slow-release properties.
However, beginning in 2000, widespread reports of OxyContin® abuse surfaced. Over the past 16 years, there have been reports, frequently anecdotal, that opioid analgesic abuse has evolved into a national epidemic.
OxyContin® abusers quickly realized that they could eliminate the slow-release mechanism by chewing or crushing the tablets, thus releasing the potent pain medication all at once. Abusers can further intensify the pain-killing effects by snorting or injecting the OxyContin® powder. Tampering with OxyContin® in this manner creates a dangerously powerful analgesic stronger than morphine or heroin.
Picture Below:
NEW FORMULATION CRUSHED
VERSUS OLD FORMULA
In 1995, approved by the FDA as a sustained-release preparation of oxycodone hydrochloride and was thought to have much lower abuse potential than immediate-release oxycodone because of its slow-release properties.
However, beginning in 2000, widespread reports of OxyContin® abuse surfaced. Over the past 16 years, there have been reports, frequently anecdotal, that opioid analgesic abuse has evolved into a national epidemic.
OxyContin® abusers quickly realized that they could eliminate the slow-release mechanism by chewing or crushing the tablets, thus releasing the potent pain medication all at once. Abusers can further intensify the pain-killing effects by snorting or injecting the OxyContin® powder. Tampering with OxyContin® in this manner creates a dangerously powerful analgesic stronger than morphine or heroin.
Picture Below:
NEW FORMULATION CRUSHED
VERSUS OLD FORMULA


L A T E S T N E W S
'Endo Pharmaceutical's
Crush-Resistant Formula for Their
Opana ER Painkiller Gets
Rejected by FDA'
Crush-Resistant Formula for Their
Opana ER Painkiller Gets
Rejected by FDA'
By: Andrew Pollack ~ Jan 7, 2011 8:49 PM ET
ENDO PHARMACEUTICAL HOLDINGS, INC, said U.S. regulators rejected a formulation of its painkiller Opana ER designed to prevent tampering and abuse.
No additional clinical studies are required and the Chadds Ford , Pennsylvania-based company has begun discussions with the Food and Drug Administration over its decision about the crush- resistant drug, Endo said today in a statement.
Makers of 24 extended-release pain pills were ordered by the FDA in February 2009 to help devise a plan to minimize the risks of the products while ensuring patients kept access to the medicines. Opana and Opana ER, the extended release version of the medication, generated $230.6 million in 2009 sales for Endo, about 16 percent of its revenue, according to data compiled by Bloomberg.
Endo expects to satisfy the FDA’s concerns and file its application by mid-2011 for the drug’s approval, Ivan Gergel, Endo’s executive vice president for research and development, said in the company’s statement. “We remain focused on bringing this new formulation of Opana ER to market for the relief of moderate to severe pain in patients requiring continuous, around-the-clock opioid treatment for an extended period of time.”
Endo fell 73 cents, or 2 percent, to $35.11 at 4 p.m. New York time in Nasdaq Stock Market composite trading. The shares gained 70 percent in the past 12 months.
To contact the editor responsible for this story: Reg Gale in New York at: [email protected]
source: www.Bloomberg.com
ENDO PHARMACEUTICAL HOLDINGS, INC, said U.S. regulators rejected a formulation of its painkiller Opana ER designed to prevent tampering and abuse.
No additional clinical studies are required and the Chadds Ford , Pennsylvania-based company has begun discussions with the Food and Drug Administration over its decision about the crush- resistant drug, Endo said today in a statement.
Makers of 24 extended-release pain pills were ordered by the FDA in February 2009 to help devise a plan to minimize the risks of the products while ensuring patients kept access to the medicines. Opana and Opana ER, the extended release version of the medication, generated $230.6 million in 2009 sales for Endo, about 16 percent of its revenue, according to data compiled by Bloomberg.
Endo expects to satisfy the FDA’s concerns and file its application by mid-2011 for the drug’s approval, Ivan Gergel, Endo’s executive vice president for research and development, said in the company’s statement. “We remain focused on bringing this new formulation of Opana ER to market for the relief of moderate to severe pain in patients requiring continuous, around-the-clock opioid treatment for an extended period of time.”
Endo fell 73 cents, or 2 percent, to $35.11 at 4 p.m. New York time in Nasdaq Stock Market composite trading. The shares gained 70 percent in the past 12 months.
To contact the editor responsible for this story: Reg Gale in New York at: [email protected]
source: www.Bloomberg.com
NOW OPEN--> OPiOiD ADDiCTiON
~CLICK HERE~ & Opana Forum
~CLICK HERE~ & Opana Forum

We Want to hear your stories of addiction and/or experiences with Opana. You can remain confidential. Please email me or if you have info/videos/news relating to opana or oxymorphone I would appreciate that as well. Email to : [email protected]. THANKS!
* PHARMACOKINETIC
D a t a *
 |
BIOAVAILABILITY
10% (oral) 40% (Intranasal) 100% (IV, IM) METABOLISM Hepatic HALF-LIFE 1.3 +/- 0.7 hrs (with parenteral admin) 7.25 - 9.43 hrS (with oral admin) |

opana ER tabs
(5mg, 7.5mg, 10mg, 15mg, 20mg, 30mg, 40mg)

opana 5mg & 10mg
A QUOTE FROM The Mind of an Opana Addict:
"....It was like falling in love. I woke up each morning with that sated, slightly guilty feeling of gluttony that perhaps I was feeling too good. I would struggle to recall the minutiae of the wonderful experiences we’d had together the night before, think about Opana all day long and then burst through the door after work: Baby! How are you? I’ve missed you so! It was like that brief period of grace in a relationship when your mutual love and desire is so powerful that the two of you rack your brains for the most deviant sexual maneuvers to try because suddenly everything and anything is safe. I was not a drug addict; I was a drug’s true love." (MISHKA SHUBALY, Indie rocker) .
"....It was like falling in love. I woke up each morning with that sated, slightly guilty feeling of gluttony that perhaps I was feeling too good. I would struggle to recall the minutiae of the wonderful experiences we’d had together the night before, think about Opana all day long and then burst through the door after work: Baby! How are you? I’ve missed you so! It was like that brief period of grace in a relationship when your mutual love and desire is so powerful that the two of you rack your brains for the most deviant sexual maneuvers to try because suddenly everything and anything is safe. I was not a drug addict; I was a drug’s true love." (MISHKA SHUBALY, Indie rocker) .

OPANA ER contains oxymorphone,
which is a morphine-like opioid agonist and a
Schedule II controlled substance, with an abuse liability similar to other opioid analgesics. Oxymorphone can be abused in a manner similar to other opioid agonists,
legal or illicit.
This should be considered when prescribing
or dispensing OPANA ER in situations where
the physician or pharmacist is concerned about an increased risk of misuse, abuse, or diversion.
Opana ER is an extended-release oral formulation of oxymorphone indicated for the management of moderate to severe pain when a continuous, around-the-clock opioid analgesic is needed for an extended period of time.
Limitations of Use
Opana ER is NOT intended for use as an as
needed analgesic. Opana ER tablets are to be swallowed whole and are not to be broken, chewed, dissolved, or crushed. Taking broken, chewed, dissolved, or crushed Opana ER tablets leads to rapid release and absorption of a potentially fatal dose of oxymorphone.
Patients must not consume alcoholic beverages, or prescription or non-prescription medications containing alcohol, while on Opana ER therapy.
The co-ingestion of alcohol with Opana ER
may result in increased plasma levels and a potentially fatal overdose of oxymorphone.
Indications And Usage
Opana ER is not indicated for pain in the
immediate post-operative period if the pain
is mild, or not expected to persist for an extended period of time.
Opana ER is only indicated for post-operative
use if the patient is already receiving the drug
prior to surgery or if the post-operative pain is expected to be moderate or severe and persist for an
extended period of time.
Physicians should individualize treatment,
moving from parenteral to oral analgesics as appropriate.
For full medication guide click here: http://www.opana.com/

opana:
A BRIEF HISTORY
POSTED: Wednesday March 5, 2008
NEW YORK Press
By Matt Elzweig
Opana– a powerful painkiller that went on the market less than two years ago – is twice as strong as OxyContin, with a potential for addiction that rivals the prescription drug that has ravaged the lives of thousands of abusers.
Little is yet known about the potential for Opana abuse, because of its relatively short shelf life in the pharmaceutical marketplace. Significantly more potent than morphine, itself a powerful painkiller with potentially fatal side effects if abused, its existence has created a possible new menace for those who use pain medications for recreational purposes. Those numbers have grown significantly in recent years, as the addictive properties of prescription drugs like OxyContin and Vicodin have become better known.
In that time, reports of abuse have grown widespread for OxyContin, introduced in 1995 and once known as “hillbilly heroin.” In its first six years of existence, news reports put revenues from OxyContin at nearly $3 billion for its manufacturer, Purdue Pharma. The effects of Opana are closer to those of morphine than of OxyContin, doctors say. Whereas OxyContin has a more stimulating effect, Opana can cause a user to fall asleep. Like morphine, Opana’s greatest danger to abusers is the possibility of “respiratory depression,” or reduced lung functioning. As with all prescription painkillers, the addictive properties of Opana present another possible danger, especially to recreational users.
According to James Zacny, a professor of anesthesia and critical care at the University of Chicago, users could eventually become physically dependent on the drug, depending on dosage and frequency of administration.
Why did Opana get introduced now?
Its manufacturer, Endo Pharmaceuticals, said the drug was developed in part to provide an alternative to patients who’ve developed a tolerance for a specific painkiller. But an Endo spokesman also cited Opana’s added benefit to patients as a “true” twice-a-day opioid. He suggested that while OxyContin is advertised as a 12-hour medication, its users “tend” to take OxyContin more frequently. Doctors say that excessive doses of OxyContin can lead to abuse. A spokesman for Purdue Pharma, the makers of OxyContin, took issue with Endo’s assessment. “OxyContin is indeed a true 12-hour medication,” he said. “All of our clinical studies were conducted using the medication at 12 hour intervals and the product was both safe and effective." But the main reason for the drug’s arrival in the marketplace may be yet more simple: the market for prescription painkillers grows with every passing day.
An injectible form of the drug – known under the generic name of oxymorphone hydrochloride – has been available since 1959, but was available only as a intravenous drip to hospitals. The oral form was originally approved by the Food and Drug Administratin
in 5, 10, 20 and 40mg extended release tablets, and immediate release tablets in 5 and 10 milligram doses. On March 3, the FDA approved three additional doses. The Opana pill has a waxy consistency designed to deter users from crushing it into a powder, which would defeat the timing mechanism if snorted.
The drug’s warning label specifically cautions users not to break the tablets down before ingesting orally, because it “leads to the rapid release and absorption of a potentially fatal dose of oxymorphone.” This isn’t the first time oxymorphone-hydrochl
oride has been available in tablet form. Until it was taken off in the market in the 1970s, it was available in 10 milligram tablets under the brand name Numorphan. That was the drug referred to as “blues” in the 1989 Gus Van Sant film, “Drugstore Cowboy,” about a family of traveling drug addicts set in the early 1970s.
SOURCE: http://www.nypress.com/article-18005-opana-a-brief-history.html
A BRIEF HISTORY
POSTED: Wednesday March 5, 2008
NEW YORK Press
By Matt Elzweig
Opana– a powerful painkiller that went on the market less than two years ago – is twice as strong as OxyContin, with a potential for addiction that rivals the prescription drug that has ravaged the lives of thousands of abusers.
Little is yet known about the potential for Opana abuse, because of its relatively short shelf life in the pharmaceutical marketplace. Significantly more potent than morphine, itself a powerful painkiller with potentially fatal side effects if abused, its existence has created a possible new menace for those who use pain medications for recreational purposes. Those numbers have grown significantly in recent years, as the addictive properties of prescription drugs like OxyContin and Vicodin have become better known.
In that time, reports of abuse have grown widespread for OxyContin, introduced in 1995 and once known as “hillbilly heroin.” In its first six years of existence, news reports put revenues from OxyContin at nearly $3 billion for its manufacturer, Purdue Pharma. The effects of Opana are closer to those of morphine than of OxyContin, doctors say. Whereas OxyContin has a more stimulating effect, Opana can cause a user to fall asleep. Like morphine, Opana’s greatest danger to abusers is the possibility of “respiratory depression,” or reduced lung functioning. As with all prescription painkillers, the addictive properties of Opana present another possible danger, especially to recreational users.
According to James Zacny, a professor of anesthesia and critical care at the University of Chicago, users could eventually become physically dependent on the drug, depending on dosage and frequency of administration.
Why did Opana get introduced now?
Its manufacturer, Endo Pharmaceuticals, said the drug was developed in part to provide an alternative to patients who’ve developed a tolerance for a specific painkiller. But an Endo spokesman also cited Opana’s added benefit to patients as a “true” twice-a-day opioid. He suggested that while OxyContin is advertised as a 12-hour medication, its users “tend” to take OxyContin more frequently. Doctors say that excessive doses of OxyContin can lead to abuse. A spokesman for Purdue Pharma, the makers of OxyContin, took issue with Endo’s assessment. “OxyContin is indeed a true 12-hour medication,” he said. “All of our clinical studies were conducted using the medication at 12 hour intervals and the product was both safe and effective." But the main reason for the drug’s arrival in the marketplace may be yet more simple: the market for prescription painkillers grows with every passing day.
An injectible form of the drug – known under the generic name of oxymorphone hydrochloride – has been available since 1959, but was available only as a intravenous drip to hospitals. The oral form was originally approved by the Food and Drug Administratin
in 5, 10, 20 and 40mg extended release tablets, and immediate release tablets in 5 and 10 milligram doses. On March 3, the FDA approved three additional doses. The Opana pill has a waxy consistency designed to deter users from crushing it into a powder, which would defeat the timing mechanism if snorted.
The drug’s warning label specifically cautions users not to break the tablets down before ingesting orally, because it “leads to the rapid release and absorption of a potentially fatal dose of oxymorphone.” This isn’t the first time oxymorphone-hydrochl
oride has been available in tablet form. Until it was taken off in the market in the 1970s, it was available in 10 milligram tablets under the brand name Numorphan. That was the drug referred to as “blues” in the 1989 Gus Van Sant film, “Drugstore Cowboy,” about a family of traveling drug addicts set in the early 1970s.
SOURCE: http://www.nypress.com/article-18005-opana-a-brief-history.html
........................................................

Crushable
~Pain Medication~
Target
for
Abuse'
POSTED: Tuesday, August 16, 2011
Police say another prescription pain reliever is gaining popularity among abusers in the Kanawha Valley. Authorities are finding more people abusing prescription Opana, a drug that appeared on officers' radars after OxyContin was reformulated late last year, said Charleston Lt. Chad Napier, commander of the Metro Drug Unit.
Because abusers of OxyContin often crush the pills and then snort them, Purdue Pharma, the manufacturer, changed the chemical makeup of the pills to include a gel coating, making them impossible to crush.
Opana, a time-release pain reliever made by Endo pharmaceuticals is not available in gel-cap form. It contains oxymorphone, which is a Schedule II controlled substance, according to the company's website. The tablet is meant for patients with around-the-clock pain and is to be swallowed whole to give the patient time-released pain relief.
The website said the drug could be abused like similar opiates and asks physicians and pharmacists to consider that when dispensing pills. Calls to the company were not returned.
"They really like the Opana," Napier said of abusers. "They say it's better than OxyContin and they get higher off of it."Mike O'Neil, chairman of the West Virginia Controlled Substances Advisory Board and president of the state chapter of the National Association of Drug Diversion Investigators, said some doctors started prescribing Opana to avoid the negative connotations associated with OxyContin.
"The use of Opana started slowly climbing because Purdue Pharma was getting such bad press with the asset forfeitures and abuse statistics," O'Neil said.
"The people running these pill mills were trying to fly under the radar by prescribing Opana because it wasn't being prescribed very often. "Despite its appeal to drug abusers, he said Opana is a good pain reliever for those with chronic pain.
"Opana is equally as potent if not more so than oxycodone," O'Neil said. "It's a good drug. It's a safe drug -- very potent -- and it works for those needing relief from pain."While Opana abuse may be on the rise in the Kanawha Valley, the abuse rate of Lortab and Xanax is far greater in West Virginia and across the country, O'Neil said.
Lortab, another prescription pain medication, and Xanax, which is used to treat patients with anxiety disorders, are ranked 1 and 2 as far as abuse.Napier said officers still are seeing generic oxycodone tablets on the streets, but Opana and Roxicodone, which also contains oxycodone, are gaining in popularity.
"They're going to crush (Opana and Roxycodone) and get the same thing they were getting before with the OxyContin," Napier said. "Judging by how popular those are, we could go out and find it every day."O'Neil said other manufacturers are beginning to move toward reformulating their products to make them tamper-resistant now that Purdue Pharma has done so with OxyContin.
Cost has been an issue.
"Its not a cheap thing to do," O'Neil said. "It's like saying how many wrecks have to occur at an intersection before they put up a traffic light when the problem is really the economics of the traffic light. "It's not really (pharmaceutical companies') main focus now; nor is it mandated by federal law."Napier said reformulating pain medications to make them tamper resistant would help police keep the pills off the streets.
U.S. Attorney Booth Goodwin said it was unfortunate that other drug makers hadn't followed suit in making their prescription opiates tamper-resistant. He has noticed more cases involving Roxicodone and Opana coming through his office."This illustrates a challenge we face in enforcement: once we get a handle on controlling the supply of one abused prescription drug, the dealers and abusers shift to another," Goodwin said."That is yet another reason why we have to attack the prescription drug crisis on all fronts through education, monitoring, proper disposal and enforcement." State government officials, medical professionals and law enforcement workers met in February for a one-day summit on the prescription drug abuse problem in West Virginia.
They talked about OxyContin, Vicodin and Xanex as problems but also noted that Opana usage was on the rise, according to a report released last week about the summit. The report indicated that West Virginia has the highest overdose death rate per capita in the nation and nine of 10 deaths could be traced back to prescription drug abuse.
The report also called prescription drug abuse the No. 1 crime problem in Southern West Virginia.
To see more of the Charleston Daily Mail, or to subscribe to the newspaper, goto http://www.dailymail.com/
Copyright (c) 2011, Charleston Daily Mail, W.Va.
Police say another prescription pain reliever is gaining popularity among abusers in the Kanawha Valley. Authorities are finding more people abusing prescription Opana, a drug that appeared on officers' radars after OxyContin was reformulated late last year, said Charleston Lt. Chad Napier, commander of the Metro Drug Unit.
Because abusers of OxyContin often crush the pills and then snort them, Purdue Pharma, the manufacturer, changed the chemical makeup of the pills to include a gel coating, making them impossible to crush.
Opana, a time-release pain reliever made by Endo pharmaceuticals is not available in gel-cap form. It contains oxymorphone, which is a Schedule II controlled substance, according to the company's website. The tablet is meant for patients with around-the-clock pain and is to be swallowed whole to give the patient time-released pain relief.
The website said the drug could be abused like similar opiates and asks physicians and pharmacists to consider that when dispensing pills. Calls to the company were not returned.
"They really like the Opana," Napier said of abusers. "They say it's better than OxyContin and they get higher off of it."Mike O'Neil, chairman of the West Virginia Controlled Substances Advisory Board and president of the state chapter of the National Association of Drug Diversion Investigators, said some doctors started prescribing Opana to avoid the negative connotations associated with OxyContin.
"The use of Opana started slowly climbing because Purdue Pharma was getting such bad press with the asset forfeitures and abuse statistics," O'Neil said.
"The people running these pill mills were trying to fly under the radar by prescribing Opana because it wasn't being prescribed very often. "Despite its appeal to drug abusers, he said Opana is a good pain reliever for those with chronic pain.
"Opana is equally as potent if not more so than oxycodone," O'Neil said. "It's a good drug. It's a safe drug -- very potent -- and it works for those needing relief from pain."While Opana abuse may be on the rise in the Kanawha Valley, the abuse rate of Lortab and Xanax is far greater in West Virginia and across the country, O'Neil said.
Lortab, another prescription pain medication, and Xanax, which is used to treat patients with anxiety disorders, are ranked 1 and 2 as far as abuse.Napier said officers still are seeing generic oxycodone tablets on the streets, but Opana and Roxicodone, which also contains oxycodone, are gaining in popularity.
"They're going to crush (Opana and Roxycodone) and get the same thing they were getting before with the OxyContin," Napier said. "Judging by how popular those are, we could go out and find it every day."O'Neil said other manufacturers are beginning to move toward reformulating their products to make them tamper-resistant now that Purdue Pharma has done so with OxyContin.
Cost has been an issue.
"Its not a cheap thing to do," O'Neil said. "It's like saying how many wrecks have to occur at an intersection before they put up a traffic light when the problem is really the economics of the traffic light. "It's not really (pharmaceutical companies') main focus now; nor is it mandated by federal law."Napier said reformulating pain medications to make them tamper resistant would help police keep the pills off the streets.
U.S. Attorney Booth Goodwin said it was unfortunate that other drug makers hadn't followed suit in making their prescription opiates tamper-resistant. He has noticed more cases involving Roxicodone and Opana coming through his office."This illustrates a challenge we face in enforcement: once we get a handle on controlling the supply of one abused prescription drug, the dealers and abusers shift to another," Goodwin said."That is yet another reason why we have to attack the prescription drug crisis on all fronts through education, monitoring, proper disposal and enforcement." State government officials, medical professionals and law enforcement workers met in February for a one-day summit on the prescription drug abuse problem in West Virginia.
They talked about OxyContin, Vicodin and Xanex as problems but also noted that Opana usage was on the rise, according to a report released last week about the summit. The report indicated that West Virginia has the highest overdose death rate per capita in the nation and nine of 10 deaths could be traced back to prescription drug abuse.
The report also called prescription drug abuse the No. 1 crime problem in Southern West Virginia.
To see more of the Charleston Daily Mail, or to subscribe to the newspaper, goto http://www.dailymail.com/
Copyright (c) 2011, Charleston Daily Mail, W.Va.
Vanguard Presents:
G A T E W A Y T O H E R O I N
G A T E W A Y T O H E R O I N
If Your Having problems viewing this entire video, it can be watched in Full on Hulu, LINK BELOW:
http://www.hulu.com/watch/249652/vanguard-gateway-to-heroin
http://www.hulu.com/watch/249652/vanguard-gateway-to-heroin
.....................................................................
BY: WHAS11
WHAS11.com
Updated yesterday at 9:41 AM
Posted on February 27, 2012 at 1:18 AM
(WHAS11) – Opana is being described as the most dangerous drug of our time. Also known as Oxymophone, it’s a painkiller that addicts describe as morphine on steroids. When used correctly, you only need one pill every 12 hours to help with pain. But when it is abused, it only takes one high to get hooked.
It’s the drug that’s taking prescription pill abuse to a whole new level. In Louisville alone it has led to numerous overdoses. In 2010 there were four deaths associated with the drug and in 2011 there were 33 deaths linked to it. Louisville police say people who’ve been able to take strong prescription painkillers without being addicted are now getting hooked on Opana. Those recovering from addiction say the high off Opana is as strong as the high they can get off of a mixture of drugs in just one hit. For many, the high is stronger than meth and police say the addiction is causing more problems than when crack cocaine first hit the streets.
Opana is an opiate that addicts say is so intense that they will lie, cheat, and steal so they don’t have to deal with the withdrawal effects.
Opana became popular in 2010 when the makers of Oxycotin reformulated their pills so they couldn’t be crushed and snorted. Now the makers of Opana are promising to do the same.
In a statement an executive with Endo Pharmaceuticals says, "We firmly believe this new formulation of Opana ER, coupled with our long term commitment to awareness and education around appropriate use of opiates will benefit patients, physicians and payers."
Police say Opana mostly comes into the Kentuckiana area from Detroit and Canada from pain clinics. Doctors will write prescriptions for large quantities at these locations if you come in with enough money. And if addicts don’t have the cash, police say they will break into homes to steal whatever they can pawn off quickly for drug money. Police say some are to the point of committing crimes with other prescription drugs in order to sell those drugs to purchase Opana or make a trade for it.
In Kentuckiana, it is estimated 60 to 80 percent of home break-ins that are happening now are linked to Opana.
Opana becomes the most dangerous when people use it like they used Oxycotin; mixed with other drugs. At this point, it can become lethal. Police say they hope when the drug is reformulated that it will curb some of the crime and abuse but know another drug will soon take its place.
WHAS11.com
Updated yesterday at 9:41 AM
Posted on February 27, 2012 at 1:18 AM
(WHAS11) – Opana is being described as the most dangerous drug of our time. Also known as Oxymophone, it’s a painkiller that addicts describe as morphine on steroids. When used correctly, you only need one pill every 12 hours to help with pain. But when it is abused, it only takes one high to get hooked.
It’s the drug that’s taking prescription pill abuse to a whole new level. In Louisville alone it has led to numerous overdoses. In 2010 there were four deaths associated with the drug and in 2011 there were 33 deaths linked to it. Louisville police say people who’ve been able to take strong prescription painkillers without being addicted are now getting hooked on Opana. Those recovering from addiction say the high off Opana is as strong as the high they can get off of a mixture of drugs in just one hit. For many, the high is stronger than meth and police say the addiction is causing more problems than when crack cocaine first hit the streets.
Opana is an opiate that addicts say is so intense that they will lie, cheat, and steal so they don’t have to deal with the withdrawal effects.
Opana became popular in 2010 when the makers of Oxycotin reformulated their pills so they couldn’t be crushed and snorted. Now the makers of Opana are promising to do the same.
In a statement an executive with Endo Pharmaceuticals says, "We firmly believe this new formulation of Opana ER, coupled with our long term commitment to awareness and education around appropriate use of opiates will benefit patients, physicians and payers."
Police say Opana mostly comes into the Kentuckiana area from Detroit and Canada from pain clinics. Doctors will write prescriptions for large quantities at these locations if you come in with enough money. And if addicts don’t have the cash, police say they will break into homes to steal whatever they can pawn off quickly for drug money. Police say some are to the point of committing crimes with other prescription drugs in order to sell those drugs to purchase Opana or make a trade for it.
In Kentuckiana, it is estimated 60 to 80 percent of home break-ins that are happening now are linked to Opana.
Opana becomes the most dangerous when people use it like they used Oxycotin; mixed with other drugs. At this point, it can become lethal. Police say they hope when the drug is reformulated that it will curb some of the crime and abuse but know another drug will soon take its place.
.
PAINKILLER, OPANA, NEW SCOURGE OF RURAL AMERICA

By Mary Wisniewski
AUSTIN, Indiana | Tue Mar 27, 2012 2:48am EDT
AUSTIN, Indiana (Reuters) - Back in high school in Houston, Texas, C.J. Coomer got good grades and played football. He was dark-haired and handsome, popular with his friends and doted on by his family.
But when his mother got divorced and moved to be near family in rural Scott County, Indiana, Coomer began running with a crowd there that abused prescription painkillers to get high. His weight dropped from 210 pounds to just 140 pounds (64 kg), he couldn't work, and was constantly borrowing money.
One night last July, Coomer tried something new -- Opana, a powerful opioid painkiller containing oxymorphone. He overdosed and died at the age of 24.
"It's a nightmare every single day," said his mother, Melissa Himmelheber, 43, who wiped away tears as she showed pictures of her lost son. "This is a family that was extremely close. Now we're just picking up the shattered pieces."
Prescription drug abuse is the new scourge of rural America. It now leads to more deaths in the United States than heroin and cocaine combined, and rural residents are nearly twice as likely to overdose on pills than people in big cities, according to the Centers for Disease Control.
While methamphetamine addiction has long been associated with small towns, prescription painkillers have overtaken meth as the most abused drugs in places such as southern Indiana, according to local authorities.
Opana is the hot new prescription drug of abuse, sometimes with tragic consequences.
At least nine people have died so far this year from prescription drug overdoses in Scott County, Indiana. Most of the fatalities involved Opana, according to county coroner Kevin Collins.
Before 2011, only about 20 percent of the cases referred to the coroner were overdose deaths, and most of those were suicides rather than accidents. Last year, prescription drug overdoses accounted for 19 deaths, or about half of all deaths referred to the coroner in this county of just 24,000 on the southern tip of Indiana, about 30 miles from Louisville, Kentucky.
"We're seeing a lot of 25-year-olds who are dead for no apparent reason," said Collins, who is so disheartened by the overdoses that it is one reason he won't run for reelection in May.
POTENT, DEADLY
Law enforcement officials are alarmed by the rise of Opana abuse, which they said started after Oxycontin was changed in late 2010 to make that drug more difficult to snort or inject for a heroin-like high. Oxycontin is a brand of oxycodone.
Opana abuse can be deadly because it is more potent, per milligram, than Oxycontin, and users who are not familiar with how strong it is may be vulnerable to overdosing.
Opana, known by such street names as "stop signs," "the O bomb," and "new blues," is crushed and either snorted or injected. Crushing defeats the pill's "extended release" design, releasing the drug all at once.
"This Opana pill has really kicked us in the rear," said Indiana State Police Sergeant Jerry Goodin. "We've never seen an addiction like this."
Oxycontin's new pills make it harder to crush them into a powder as they instead become gummy and cannot be readily snorted or injected. This drove abusers to switch to Opana or to generic, immediate-release forms of oxycodone, according to John Burke, president of the National Association of Drug Diversion Investigators. Drug abuse experts have also found an increase in heroin use.
Endo Pharmaceuticals, which produces Opana, announced in December that it would reformulate Opana. The new pill is being manufactured now.
The new formulation makes it difficult to crush and it turns viscous or "gooey" if an abuser tries to add liquid to it, said company spokesman Kevin Wiggins. When used properly, Opana is indicated for chronic low back and osteoarthritis pain, and cancer pain.
But the old form of Opana is still available, and pharmacy and home robberies are on the rise as addicts search for a way to get their fix, according to police.
"We're pretty much consumed by it," Shane McHenry, a detective with the Dearborn County Sheriff's Department in southern Indiana, said of Opana. He said users who cannot afford Opana sometimes travel to Cincinnati to get heroin, which is cheaper in smaller amounts.
Fort Wayne, Indiana reported about 11 pharmacy robberies related to Opana since Endo announced the reformulation, according to Fort Wayne police spokeswoman Raquel Foster. The thief would hand the pharmacist a note, as in a bank robbery, threatening harm if Opana was not delivered.
MANY SOURCES
The Opana problem has been reported by abuse experts around the country. In Florida, for example, the number of oxymorphone-related deaths rose to 493 in 2010, an increase of 109 percent from the previous year, according to Jim Hall, director of a drug abuse center at Nova Southeastern University in Florida.
Some users and dealers get painkillers from so-called "pill mills" -- storefront pain clinics that sell drugs for cash up front, often to out of-state buyers who take them for resale.
But the other way users get pills is from their doctors, or by buying from seniors looking to supplement a fixed income. One Opana pill brings up to $90 on the street depending on dosage, so it is tempting to sell, said Scott County Sheriff Dan McClain.
A woman in her late 70s was arrested in Austin, Indiana for exchanging pills for work around her house, McClain said.
"Most of what I see is people with a prescription from their doctors and they need the money," said Austin, Indiana Police Detective Lonnie Noble. He said the appetite for Opana is "more aggressive" than it was for Oxycontin.
Nashville, Tennessee Detective Michael Donaldson, who also has seen an increase in Opana abuse, said many small towns have "dirty doctors" willing to give out unneeded prescriptions.
Scott County is one of the poorest areas in Indiana, with a median household income of $39,588 in 2010. It was a hot spot for oxycodone retail distribution in 2010, with 48.79 per capita dosage units -- the highest in the state, according to Lori Croasdell, a coordinator for CEASe of Scott County, a drug abuse prevention group.
A northern section of Austin in Scott County showed signs of poverty and neglect. Run-down trailers and houses with broken windows and peeling paint were mixed in among well-kept homes and tidy gardens.
McClain said the drugs cause a vicious cycle of poverty, since abusers cannot hold a job. "Most of them sleep until noon, get up, and try to find a way to get another pill," said McClain.
One reason for the rise in prescription pill abuse is that Americans feel they can fix any problem - pain, depression, anxiety, hopelessness - with a pill, according to Shane Avery, a Scott County doctor. And some doctors, who may mean well but fear being sued for undertreating pain, give out pills better suited for cancer patients to soothe a backache, Avery said.
"The people who abuse prescription medications know how to doctor shop," said Collins, the Scott County coroner.
(Reporting By Mary Wisniewski; Additional reporting by Tim Ghianni in Nashville, Tennesee; Editing by Greg McCune and Tim Dobbyn)
AUSTIN, Indiana | Tue Mar 27, 2012 2:48am EDT
AUSTIN, Indiana (Reuters) - Back in high school in Houston, Texas, C.J. Coomer got good grades and played football. He was dark-haired and handsome, popular with his friends and doted on by his family.
But when his mother got divorced and moved to be near family in rural Scott County, Indiana, Coomer began running with a crowd there that abused prescription painkillers to get high. His weight dropped from 210 pounds to just 140 pounds (64 kg), he couldn't work, and was constantly borrowing money.
One night last July, Coomer tried something new -- Opana, a powerful opioid painkiller containing oxymorphone. He overdosed and died at the age of 24.
"It's a nightmare every single day," said his mother, Melissa Himmelheber, 43, who wiped away tears as she showed pictures of her lost son. "This is a family that was extremely close. Now we're just picking up the shattered pieces."
Prescription drug abuse is the new scourge of rural America. It now leads to more deaths in the United States than heroin and cocaine combined, and rural residents are nearly twice as likely to overdose on pills than people in big cities, according to the Centers for Disease Control.
While methamphetamine addiction has long been associated with small towns, prescription painkillers have overtaken meth as the most abused drugs in places such as southern Indiana, according to local authorities.
Opana is the hot new prescription drug of abuse, sometimes with tragic consequences.
At least nine people have died so far this year from prescription drug overdoses in Scott County, Indiana. Most of the fatalities involved Opana, according to county coroner Kevin Collins.
Before 2011, only about 20 percent of the cases referred to the coroner were overdose deaths, and most of those were suicides rather than accidents. Last year, prescription drug overdoses accounted for 19 deaths, or about half of all deaths referred to the coroner in this county of just 24,000 on the southern tip of Indiana, about 30 miles from Louisville, Kentucky.
"We're seeing a lot of 25-year-olds who are dead for no apparent reason," said Collins, who is so disheartened by the overdoses that it is one reason he won't run for reelection in May.
POTENT, DEADLY
Law enforcement officials are alarmed by the rise of Opana abuse, which they said started after Oxycontin was changed in late 2010 to make that drug more difficult to snort or inject for a heroin-like high. Oxycontin is a brand of oxycodone.
Opana abuse can be deadly because it is more potent, per milligram, than Oxycontin, and users who are not familiar with how strong it is may be vulnerable to overdosing.
Opana, known by such street names as "stop signs," "the O bomb," and "new blues," is crushed and either snorted or injected. Crushing defeats the pill's "extended release" design, releasing the drug all at once.
"This Opana pill has really kicked us in the rear," said Indiana State Police Sergeant Jerry Goodin. "We've never seen an addiction like this."
Oxycontin's new pills make it harder to crush them into a powder as they instead become gummy and cannot be readily snorted or injected. This drove abusers to switch to Opana or to generic, immediate-release forms of oxycodone, according to John Burke, president of the National Association of Drug Diversion Investigators. Drug abuse experts have also found an increase in heroin use.
Endo Pharmaceuticals, which produces Opana, announced in December that it would reformulate Opana. The new pill is being manufactured now.
The new formulation makes it difficult to crush and it turns viscous or "gooey" if an abuser tries to add liquid to it, said company spokesman Kevin Wiggins. When used properly, Opana is indicated for chronic low back and osteoarthritis pain, and cancer pain.
But the old form of Opana is still available, and pharmacy and home robberies are on the rise as addicts search for a way to get their fix, according to police.
"We're pretty much consumed by it," Shane McHenry, a detective with the Dearborn County Sheriff's Department in southern Indiana, said of Opana. He said users who cannot afford Opana sometimes travel to Cincinnati to get heroin, which is cheaper in smaller amounts.
Fort Wayne, Indiana reported about 11 pharmacy robberies related to Opana since Endo announced the reformulation, according to Fort Wayne police spokeswoman Raquel Foster. The thief would hand the pharmacist a note, as in a bank robbery, threatening harm if Opana was not delivered.
MANY SOURCES
The Opana problem has been reported by abuse experts around the country. In Florida, for example, the number of oxymorphone-related deaths rose to 493 in 2010, an increase of 109 percent from the previous year, according to Jim Hall, director of a drug abuse center at Nova Southeastern University in Florida.
Some users and dealers get painkillers from so-called "pill mills" -- storefront pain clinics that sell drugs for cash up front, often to out of-state buyers who take them for resale.
But the other way users get pills is from their doctors, or by buying from seniors looking to supplement a fixed income. One Opana pill brings up to $90 on the street depending on dosage, so it is tempting to sell, said Scott County Sheriff Dan McClain.
A woman in her late 70s was arrested in Austin, Indiana for exchanging pills for work around her house, McClain said.
"Most of what I see is people with a prescription from their doctors and they need the money," said Austin, Indiana Police Detective Lonnie Noble. He said the appetite for Opana is "more aggressive" than it was for Oxycontin.
Nashville, Tennessee Detective Michael Donaldson, who also has seen an increase in Opana abuse, said many small towns have "dirty doctors" willing to give out unneeded prescriptions.
Scott County is one of the poorest areas in Indiana, with a median household income of $39,588 in 2010. It was a hot spot for oxycodone retail distribution in 2010, with 48.79 per capita dosage units -- the highest in the state, according to Lori Croasdell, a coordinator for CEASe of Scott County, a drug abuse prevention group.
A northern section of Austin in Scott County showed signs of poverty and neglect. Run-down trailers and houses with broken windows and peeling paint were mixed in among well-kept homes and tidy gardens.
McClain said the drugs cause a vicious cycle of poverty, since abusers cannot hold a job. "Most of them sleep until noon, get up, and try to find a way to get another pill," said McClain.
One reason for the rise in prescription pill abuse is that Americans feel they can fix any problem - pain, depression, anxiety, hopelessness - with a pill, according to Shane Avery, a Scott County doctor. And some doctors, who may mean well but fear being sued for undertreating pain, give out pills better suited for cancer patients to soothe a backache, Avery said.
"The people who abuse prescription medications know how to doctor shop," said Collins, the Scott County coroner.
(Reporting By Mary Wisniewski; Additional reporting by Tim Ghianni in Nashville, Tennesee; Editing by Greg McCune and Tim Dobbyn)

|
more information --> about opana This prescription medication is a narcotic and meant for treating moderate to severe pain. It’s the generic name for medications including Opana, Opana ER and Numorphan HCI. Oxymorphone is said to act similar to morphine. Opana ER is the extended release version and used to treat moderate to severe, around-the-clock pain. Oxymorphone works by attaching to receptors in the brain and nervous system to block pain. One of the most important things to know about oxymorphone and other potent narcotic analgesics is that they can be habit-forming. It is also considered a drug of abuse and can lead to problems including the development of tolerance, physical and psychological addiction, abuse, overdose, withdrawal symptoms and the need for medical detox. Oxymorphone is not for everyone so you should check the product’s instructions on use before taking it. It can interact with other medications and medical conditions. It’s essential to take oxymorphone only as prescribed. Taking it more often than prescribed or recommended or in higher doses could lead to dependence or overdose. Important Safety Information : When Taking Oxymorphone This opiate medication should be taken cautiously. Because it can cause drowsiness, dizziness and light headed feelings, it should not be taken with alcohol, other narcotics and certain other meds . The combination of oxymorphone and other substances could heighten side effects. The elderly may be more sensitive to side effects and the effectiveness of oxymorphone has not been established in children under 18. The drug may cause harm to a fetus so pregnant women should talk to their doctors and weigh the benefits and risks. Misuse or abuse of the drug can lead to serious side effects including:
____________________________________________________ 1-855-DRUGFREE (1-855-378-4373) is toll-free, national Helpline. |
|
|
|
|
Disclaimer: The contents of OpioidAddiction.weebly.com/HALO inc. are for general informational purposes only and are not intended to substitute for professional or medical evaluation, diagnosis, treatment, or advice. Users of this site are encouraged to contact your professional healthcare provider for medical assistance regarding addictive disorders, general health problems, mental health problems, and any & all health-related questions.
